what is difference between IDC and DCIS?
- how does IDC present?
- most common look on mammo?
answer
DCIS is confined to the duct and IDC invades through the duct
- most commonly presents as a hard, non-mobile, painless mass
- Mammo: irregular, high density mass with indistinct or spiculated margins
question
what is the most common subtype of IDC?
- second most common?
answer
Invasive Ductal NOS (65%)
= papillary subtype is second most common
what does tubular IDC look like on imaging?
- association on imaging?
- contralateral breast in tubular ca has __% risk of also having cancer
answer
Tubular IDC:
- spiculated slow growing mass
- favorable prognosis
- associated with a RADIAL SCAR
Contralateral breast: 10-15% cancer
question
round or lobulated circumscribed mass that is T2 bright = what IDC subtype
answer
mucinous IDC
- well circumscribed mass on mammo
- T2 bright on MRI
question
medullary ca is associated with which genetic predisposition
answer
BRCA1
question
axillary nodes (common/uncommon) with medullary breast cancer
answer
common
- axillary nodes can be Large even in the absence of mets
question
axillary nodes (common/uncommon) with papillary breast cancer
answer
uncommon
question
which subtype of IDC has a complex cystic and solid appearance
answer
Papillary IDC
question
what is the difference between Multifocal and Multicentric breast cancer?
answer
Multifocal: Multiple primaries in a FOCAL area (same quadrant)
- less than 4-5 cm apart
Multicentric: Multiple primaries scattered through the breast (different quadrants)
- multiple discrete unrelated centers of cancer
question
what is the "earliest form of breast cancer"
answer
DCIS - cancer confined to the duct
question
what does DCIS look like on galactogram?
answer
multiple intraductal filling defects in affected duct
question
the (comedo/non-comedo) type of DCIS is more aggressive
answer
Comedo type is more aggressive
question
__% of DCIS on imaging may have invasive component at time of bx
answer
10%
question
___% of DCIS on core bx may have an invasive component on surgical excision
answer
25%
question
__% of DCIS will present as a mass w/o calcs
answer
8%
question
if untreated, DICS has risk of __% of progression to invasive cancers per year
answer
1% per year
question
what 3 ways can they show DCIS convincingly?
answer
- suspcious calcs (fine linear branching or fine pleomorphic)
- NMLE on MRI
- multiple intraductal masses on galactography
question
what is the second most common type of breast cancer?
- what % of all breast cancer?
answer
invasive LOBULAR carcinoma
- 5-10% of all breast cancers
question
in lobular cancer cells, they lose ____ (etiology)
answer
e-cadherin, so they no longer stick to each other and infiltrate the breast
- infiltrate the breast like "the web of a spider"
question
how does ILC look on mammogram?
- any buzzwords?
answer
Mammo:
- architectural distortion without a central mass on a single view (typically the CC)
- "dark star"
question
how does ILC look on US?
answer
ill defined area of shadowing without a mass
question
shrinking breast = ____
- why does it have this appearance?
answer
ILC
- breast is not actually smaller, it just doesn't compress as much
question
DDX for architectural distortion without a central mass (4)
answer
Dark Star:
- lobular ca
- radial scar
- surgical scar
- IDC-NOS
question
IDC vs ILC; which is more common:
- multifocal and bilateral
- met to axilla
- met to strange places (peritoneal surface)
- calcifications
- positive margins
- treated with mastectomy more often
answer
ILC:
- more often multifocal and bilateral
- mets to strange places
- positive margins
- treated with mastectomy
IDC:
- more often mets to axilla
- more often has calcs
question
Inflammatory breast cancer:
- how does it present?
- mammo buzzword
- treatment?
- prognosis?
answer
- presents as a swollen red breast
- "skin thickening" on mammo
- chemotherapy done prior to surgery; mastectomy is still done
- prognosis is terrible
question
what is Pagets?
- what is the stage of the cancer?
answer
carcinoma in situ of the nipple epidermis
- only 50% will have palpable finding associated with the skin changes
- pagets is NOT considered T4: skin involvement does not up the stage
question
what is pagets associated with?
answer
high grade DCIS
question
T/F: Wedge biopsy should be done on any skin lesion that affects the nipple-areolar complex that doesn't resolve with topical therapy.
answer
True
question
6 high risk breast lesions
answer
"the PPARLAr is dangerous"
1. Atypical Ductal Hyperplasia (ADH)
2. Atypical Lobular Hyperplasia (ALH)
3. Lobular Carcinoma In Situ (LCIS)
4. radial scar
5. papilloma
6. phyllodes
question
Radial scar:
- what is it and what does it look like
- what 2 main cancers is it associated with
answer
dense fibrosis around the ducts, giving appearance of architectural distortion
Associated CA
- Tubular IDC
- DCIS and/or IDC 10-30%
question
what is ADH?
answer
basically DCIS but lacks quantitiatve definiton by histology (< 2 ducts involved)
question
__% of time, ADH is upgraded to DCIS on surgical path after excision
answer
30%
question
Buzzword for LCIS?
how much higher of risk is LCIS for cancer?
answer
"incidental finding" - classically occult on mammogram
- 11x higher risk for cancer
question
risk of breast cancer with ALH?
answer
4-5x higher
question
how are LCIS and ALH different?
answer
LCIS has a distended lobule
- ALH does not
question
most common intraductal mass lesion = _____
answer
papilloma
question
most common cause of bloody nipple discharge?
answer
papilloma
question
Papilloma:
- age?
- location?
how does it look on mammo, US, galactography?
answer
- usually around 50s
- classically in subareolar region
- Mammo: normal (may show calcs)
- US: Well defined smooth walled hypo-echoic mass; may have cystic and solid components and associated duct dilation
- Galactography: solitary filling defect with a dilated duct
question
phylloides has malignant degeneration in ___%
answer
10
- phylloides is fast growing
question
what BR is multiple bilateral well circumscribed masses without suspicious features
answer
BR2
- multiple means at least 3
question
when is breast pain worse in the menstrual cycle?
answer
luteal phase (increased progesterone and density)
question
combined mammo and US for "focal pain" has negative predictive value of
what are some causes of non-focal skin thickening/breast edema
answer
benign conditions
- CHF
- renal failure
*trabecular thickening on mammo (favoring dependent portion of breast)
question
DDx for unilateral swollen red breast?
answer
- mastitis
- inflammatory breast cancer
question
Mastitis:
- who is at risk
- symptoms
answer
- smokers and diabetics are at risk
- painful swollen red breast
associated with breast feeding
question
Inflammatory breast cancer:
- symptoms
- typical breast appearance
- diagnosis made?
- treatment
answer
- PAINLESS swollen red breast that does not improve with antibiotics
- breast has a "peau d'orange" appearance
- diagnosis via biopsy
- Tx: chemo/radiation, then surgery
question
what are the most suspicious features of discharge? (3)
answer
SPONTANEOUS, BLOODY discharge from a SINGLE duct
- serous (clear) discharge is also suspicious
question
is milky discharge suspicious?
- what are some causes of milky discharge? (3)
answer
Milky discharge is NOT suspicious
Causes:
- thyroid issues
- pituitary adenoma/prolactinoma
- meds (antidepressants, reglan)
Benign:
- Premenopausal: Fibrocystic change
- Postmenopausal: Ductal ectasia
Worrisome:
- Intraductal papilloma (90%): single intraductal mass near nipple
- DCIS (10%): multiple intraductal masses
question
what is the most common benign cause of benign nipple discharge in a post menopausal woman?
answer
ductal ectasia
question
how do you perform a galactography?
answer
take a 27-30 gauge blunt tipped needle and attempt to cannulate the single duct that is leaking (pt will express fluid from nipple)
- gently inject 0.2 - 0.3 mL contrast and then do mammos
question
if you see filling defects on galactogram, what do you do?
answer
wire localization
question
contraindications to galactogram? (4)
answer
1. active infxn
2. inability to express discharge
3. contrast allergy
4. prior surgery to nipple complex
question
what is architectural distortion?
answer
distortion of the normal architecture without a visible mass
- radiation of normal thin lines into a focal point
question
what is the difference between architectural distortion and summation?
answer
AD: all lines radiate to a focal point
Summation: lines continue past each other
question
how can you distinguish between surgical scar vs something bad?
answer
Scars should progressively get lighter and harder to see
- if asymmetry is increasing, you have to biopsy
question
how do you work up AD?
answer
BR 0 on screener
- if it persists on additional views, BR4 or 5 (unless a scar)
- should ultrasound it for further characterization
question
if you don't see anything on ultrasound or MRI for AD, what do you do?
answer
Biopsy it still (stereo biopsy) or seed localization for surgical excision
question
radiating lines to a single point = ____
answer
AD (architectural distortion)
question
AD + calcifications
answer
IDC + DCIS
question
AD without calcifications
answer
ILC
question
can you BR3 architectural distortion
answer
NO - even if it has been there for a while, it needs to get worked up
question
(unilateral/bilateral) axillary adenopathy should make you worried about cancer
answer
Unilateral axillary adenopathy is worrisome
question
what are the signs of an abnormal lymph node on US?
- which is most specific?
answer
- Loss of a fatty hilum (most specific)
- Cortical thickness (> 2-3mm)
- Irregular outer margins
question
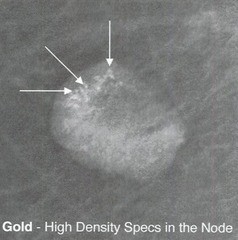
"very dense calcifications" in an axillary lymph node on mammo =
answer
- Gold therapy "chrysotherapy" (previously treated RA with gold)
question
"snow storm" lymph node =
- causes (2)
answer
Silicone infiltration of a node
- silicone implant LEAKING or RUPTURE
question
DDx for axillary mets with calcs (3)
answer
thyroid, ovarian, breast
question
Do men get lobule associated pathology?
answer
NO
- they don't get lobular carcinoma, fibroadenoma, or cysts
question
Gynecomastia:
- what is it?
- causes
- mammo look
answer
- it is a non-neoplastic enlargement of epithelial and stromal elements
Causes:
- physiologic in adolescents
- drugs (spironolactone, psych meds, marijuana)
- cirrhosis
- testicular cancer
Mammo: flame shaped, behind nipple; can be bilateral but asymmetric
- can be painful
question
type of gynecomastia that is flame shaped
answer
nodular
- most common
- painful
question
type of gynecomastia that resembles a branching tree
answer
dendritic
- non-tender
- chronic fibrotic pattern
question
type of gynecomastia that looks like women's breast = _____
- in what situation is this seen?
answer
diffuse glandular
- seen in men receiving estrogen treatment
question
what is pseudogynecomastia?
answer
increase in the fat tissue of the breast (not glandular tissue)
- NO discrete palpable finding
question
what is the most common palpable mass in a man? second most common?
answer
most common: gynecomastia
second: lipoma
question
BRCA 1/2 is more common with male breast cancer?
- what are other Risk factors? (3)
answer
BRCA 2 is more common
RFs:
- Klinefelter syndrome
- cirrhosis
- alcoholism
question
what are some things that make you suspicious for cancer in a male? (5)
answer
- eccentric to nipple
- unilateral
- abnormal lymph nodes
- calcifications (uncommon in men)
- looks like breast cancer
question
what type of cancer is found in males?
answer
IDC-NOS (by far most common)
question
T/F: males with gynecomastia from gender reassignment on hormone therapy are NOT high enough risk for screening mammograms.
answer
True
question
how do you tell difference between a saline and a silicone implant
answer
You can see through the saline implant on a mammo, silicone you can't
question
which type of implants form a capsule around it?
answer
Silicone implants form a shell around the foreign body (implant) which allows for both INTRA and EXTRA capsular rupture
- saline does not form a capsule
question
does anyone care if saline implant ruptures?
- what type of ruptures can saline have?
answer
No, saline implant rupture is NOT dangerous
- saline does not form a capsule, so cannot have an intracapsular rupture with saline
- there is only one kind of rupture
question
what happens to the saline in an implant rupture?
answer
the saline is absorbed by the body, and you have a collapsed implant
question
what kind of silicone implant rupture can you see on mammogram?
answer
can only see EXTRAcapsular rupture on mammogram
- can also see implant folds and valves
- cannot see intracapsular rupture
question
"stepladder" appearance on US means
answer
INTRAcapsular silicone implant rupture
- multiple parallel hyperechoic lines within collapsed implant shell
- corresponds to linguine sign on MRI
question
snowstorm appearance on US
answer
EXTRAcapsular rupture
question
which rupture can be isolated: intra or extra-capsular?
answer
- CAN have INTRAcapsular rupture by itself
- CANNOT have EXTRAcapsular by itself (always occurs with intracapsular rupture)
question
if silicone is seen in LN, what do you recommend as a next step
answer
MRI to look for intracapsular rupture
question
capsular contracture is most common cxc of which type of implant?
answer
subglandular silicone implants
question
what are the implant location subtpes? (2)
answer
Subglandular (retromammary)
- behind breast tissue
- anterior to pectoral muscle
Subpectoral (retropectoral)
- between pec major and minor muscles
question
what kind of implants are easier to displace for a mammogram: (subpectoral/subglandular)?
answer
subpectoral
--> better sensitivity for screening for ca
question
Do implants increase the risk of cancer?
answer
NO
question
Are implants a contraindication for core needle biopsy?
answer
NO
question
what is the most accurate modality for evaluating an implant?
answer
MRI
question
what is the most common complication of implants?
- why does it occur?
- symptom?
- what type of implant is most common?
answer
Capsular Contracture
- secondary to contraction of the fibrous capsule
- terrible cosmetic deformity
- most common in subglandular silicone implants (occurs with saline as well)
question
silicone in LNs could indicate what?
answer
gel bleed
- does not mean rupture
question
What is a Gel Bleed?
- how is it classically shown
answer
Silicone molecules can (and do) pass through the semi-pereable implant shell coating the exterior of the surface
- NOT a rupture
- will show silicone in axillary LNs
question
what are some risk factors for implant rupture? (4)
- what is the number one risk factor?
answer
- AGE of the IMPLANT is the number one risk factor
- post traumatic
- spontaneously
- rupture with compression mammography is rare
question
what is the modality to diagnose saline implant rupture?
- how will it look?
answer
Saline rupture is very obvious (deflated breast)
- will see "wadded up" plastic wrapper
- best modality is mammography (don't need ultrasound or MRI)
question
how is isolated intracapsular silicone implant rupture diagnosed?
answer
MRI is the most sensitive modality ("linguine" sign)
- can see "stepladder" on US
- will be occult on physical exam and mammography
question
how do you diagnose extracapsular silicone implant rupture?
answer
Mammogram: dense silicone seen outside the capsule
- "snow storm" US appearance: really echogenic with no posterior shadowing
- MRI: extracapsular silicone will be T1 dark and T2 bright
question
can you have isolated extracapsular rupture?
answer
NO
question
what are radial folds? why are they important?
answer
Radial folds are the normal in-foldings of the elastomer shell
- can mimic linguine sign of intracapsular rupture
question
how do you tell them apart from linguine sign?
answer
Folds ALWAYS attach to the shell of implant
- folds are thicker than rupture
question
Overview Intracapsular Rupture:
- what is the capsule?
- solitary?
- classic sign
answer
Capsule is the fibrous coat body makes around implant
- CAN rupture through shell of implant, confined within fibrous coat
- "linguine sign" on MRI
question
Overview Extracapsular rupture:
- what is it
- isolated?
- classic sign?
answer
when rupture goes THROUGH the fibrous capsule your body makes
- CANNOT have isolated extra (if it went through the outer, it also went through the inner)
- "snow storm" on ultrasound (can also be gel bleed)
question
surgery that is done to reduce breast size = _____
answer
reduction mammoplasty
question
what is a mastopexy?
- what is the imaging appearance of mastopexy?
answer
a "breast lift"
- just removal of skin to address floppy "ptotic" breasts
- swirled appearance affecting inferior breast
- fat necrosis/oil cysts
- isolated islands of breast tissue
question
in what situations is a "keyhole incision" done? (2)
answer
- mammoplasty
- mastopexy
"swirled" appearance in the inferior aspect of the MLO view
question
what are the definitions of the following:
- lumpectomy
- excisional biopsy
- incisional biopsy
answer
Lumpectomy: surgical removal of cancer
Excisional biopsy: surgical removal of the ENTIRE lesion
Incisional biopsy: surgical removal of a PORTION of the lesion
question
when should distortion and scarring be the worst on mammogram after surgery?
answer
Distortion and scarring are worst on the first post-operative mammogram and should progressively improve
- First mammo normally done 6-12 months postop
question
how should scars look on mammogram?
answer
Scars should be thin and linear
- if you see focal mass-like thickening, that is suspicious
- fat necrosis and dystrophic calcs may evolve over the first year or two
question
local recurrence occurs ____% of time when women have breast conserving therapy
answer
6-8%
question
when is peak time for recurrence
answer
4yrs
question
without radiation, local is recurrence is __%
answer
35%
question
Risk factors for recurrence (6)
answer
1. PREMENOPAUSAL WOMEN (genetic issues)
2. extensive inarticulate component
3. tumor with vascular invasion
4. multicentric tumors
5. positive surgical margins
6. inadequate treatment of first tumor
question
residual calcs in lumpectomy bed means __% local recurrence
answer
60%
question
after cancer, benign calcs occur at ___ yrs, malignant calcs come back at ___ yrs
answer
benign calcs: 2 years (early)
bad calcs: 4 yrs (late)
question
how often does sentinel node biopsy work?
answer
95% of the time it works
question
when a surgical TRAM flap is used, where is the cancer going to recur?
answer
Recurrence is from residual breast tissue or along the skin scar line
- NOT going to start in belly fat/muscle
question
On a specimen radiograph what are 2 things you need to look at?
answer
- mass/calcs included in the sample
- mass/calcs near the edge or touching the edge
question
if the mass is near the edge of specimen, what should you do? why is this important?
answer
call the surgeon because chance of incomplete excision is 80%
question
why is evaluation of the pre-radiation mammogram very important?
answer
identification of residual disease prior to radiation give the patient more treatment options
- discovery of residual disease after radiation therapy has started --> pt has to undergo mastectomy
question
what are typical radiation changes you can see on the mammogram?
- when should these changes peak?
answer
Skin thickening and trabecular thickening
- peak on first post-RT mammogram
question
what doe this sequence of mammograms mean?
- film 1 (post radiation): skin and trabecular thick
- film 2: thickening is better
- film 3: thickening is worse
answer
Recurrent disease!
- may be inflammatory breast CA
question
Breast cancer staging:
- T1
- T2
- T3
- T4
answer
T1: < 2cm
T2: 2-5 cm
T3: > 5 cm
T4: any size with chest wall fixation, skin involvement, or inflammatory breast cancer
question
is Pagets considered T4 since there is skin involvement
answer
no
question
what is the most important predictor of overall survival in breast cancer
answer
axillary status
question
what is the most common tumor to met to the breast
answer
melanoma
question
contraindications for breast conservation therapy (5)
answer
1. inflammatory cancer
2. large cancer size relative to breast
3. multicentric
4. prior radiation therapy to same breast
5. contraindications to radiation therapy (collagen-vascular disease)
question
what is the biggest reason for breast MRI?
- other reasons (4)
answer
HIGH RISK SCREENING (biggest)
- extent of disease (known cancer)
- axillary met with unknown primary
- possible silicone implant rupture
- diagnostic dillemas
question
In general, how is breast MRI done?
- what sequences?
answer
special breast coil and table are set up, and the patient lies belly down with breasts hanging through holes
Sequences:
- T2
- pre and post dynamic post contrast fat sat T1
- may also get a non fat sat T1
question
what is basic approach to look at breast MRI (4 steps)
answer
1) look at background uptake (adjusts sensitivity level)
2) look for masses or foci (little dots)
- associated features such as spiculated
3) look at washout curve
- morphology of lesion trumps washout curve
4) New masses --> BR4 or 5
NMLE --> BR4 if new
T2 stuff --> BR2 mostly
question
are most T2 bright things benign or malignant?
answer
T2 things are bright
- LNs, fibroadenoma, cyst
question
who gets screening MRI (2)
answer
> 20% lifetime chance of cancer
- includes people who got 20 Gy radiation to chest as a child
question
what scale do you use to estimate risk of who is > 20% lifetime risk
answer
- use a risk model that includes family history (NOT the Gail model)
- Tyrer-Cuzick scale is probably the best
question
Is background parenchymal enhancement normal?
- where is it most common and when in menstrual cycle?
- how do you reduce it?
answer
Parenchymal enhancement is NORMAL
- most common in POSTERIOR breast in UPPER OUTER quadrant
- worst in the luteal phase (14-28 day)
- Improve: image in follicular phase of menstrual cycle (7-14)
question
how does tamoxifen affect background parenchymal enhancement
answer
decreases background
- then causes a rebound
question
how big is a "focus" in breast MR
- are they high risk
- when should you biopsy one? (3)
answer
Focus: < 5 mm
- not typically high risk
Biopsy if:
- SUSPICIOUS ENHANCEMENT
- different than the rest
- ill-defined borders
question
when can you use BIRADS 3 on MRI (1)
answer
solitary focus (< 5 mm) with persistent kinetics on baseline exam
question
what is Non-Mass Like Enhancement (NMLE)?
- different distributions (3)
- what makes this suspicious?
answer
NMLE:
not a mass, but more like a clump of tissue enhancement
Distributions:
- Segmental (triangular blob point to the nipple)
- Regional (a bigger triangle)
- Diffuse (all over the place)
Suspicious:
- HETEROGENEOUS enhancement
question
mass on MRI is what size
answer
> 5 mm
question
When are masses bad? (3)
answer
- Irregular shape
- Spiculated margin
- Heterogeneous or rim enhancement
question
which one is better to evaluate for cancer on mri: morphology or kinetics?
answer
MORPHOLOGY
- use kinetics only if you are on the fence
question
how is breast kinetics performed? (2)
answer
- intial upslope phase (occurs over the first 2 minutes); slow, medium, or fast
- the washout portion (2-6 minutes); continued rise, plateau, or rapid washout
question
type 3 kinetic curve has what characteristics on delayed?
- % risk of cancer
answer
Type 3 has washout on delayed (most worrisome)
- 29% or higher risk of cancer
question
type 1 kinetic curve has what characteristics on delayed?
- % risk of cancer
answer
has progressive enhancement on delayed
- 6% risk of cancer
question
type 2 kinetic curve has what characteristics on delayed?
- % risk of cancer
answer
has plateau of enhancement on delayed
- 7-28% risk of cancer
question
Classic look for breast lesion on MRI: what is it?
- T2 bright, round, with "non-enhancing septa"
- type 1 curve
answer
Fibroadenoma
question
Classic look for breast lesion on MRI: what is it?
- Clumped, ductal, linear or segmental NMLE
answer
DCIS
- kinetics not typically helpful
question
Classic look for breast lesion on MRI: what is it?
- Spiculated irregular shaped mass with heterogeneous enhancement
- Type 3 curve
answer
IDC
question
Classic look for breast lesion on MRI: what is it?
- doesnt always show enhancement
answer
ILC (vague findings like on mammo)
question
DDx for benign T2 bright lesions (4)
answer
- fibroadenoma
- LNs
- cyst
- fat necrosis
question
which cancers can be T2 bright (2)
answer
- colloid
- mucinous
question
known breast cancer, how often is contralateral cancer found with mammo? MRI?
answer
Mammo: 0.1 - 2%
MRI: 3 - 5%
question
T/F: Never BR-0 an MRI case.
answer
TRUE
question
spiculated margins on MRI has __% risk of cancer
answer
80%
- single most predictive feature of malignancy
question
T/F: risk of breast cancer is directly related to estrogen.
answer
True
- more estrogen --> increased risk
question
what are some estrogen related risks? (6)
answer
- Early menstruation
- Late Menopause
- late age of first pregnancy/no kids
- being fat (increased aromatose)
- alcoholism
- hormone replacement therapy
question
what are the high risk lesions which cause an increased risk of cancer? (6)
answer
"the PPARLAr is dangerous"
- Papilloma
- Phyllodes
- ALH
- Radial scar
- LCIS
- ADH
question
does breast density have any correlation with risk of breast cancer?
answer
Increased density --> increased risk
question
risk of cancer after chest wall radiation peaks at
answer
15 yrs post treatment
question
when do you start screening someone with chest wall radiation
answer
at age 25 or 8 yrs s/p exposure (whichever is LATER)
- for a kid with > 20 Gy to the chest (usually lymphoma patients)
question
first degree relative with breast cancer increases your lifetime risk for ____% to _____%.
answer
8% to 13%
question
two first degree relatives with breast cancer gives you __% risk of breast ca
answer
21%
question
BRCA1 is which chromosome
- increased risk of what other cancers?
answer
chromosome 17
- increased breast, ovary, and GI cancers
question
BRCA2 is which chromosome
answer
13
- increased breast, ovary, and GI
- male breast cancer
question
what is Li-Fraumeni?
answer
p53 does NOT work
- increased risk for a bunch of cancers
question
Cowden syndrome is at risk for what cancer? (4)
answer
breast
follicular thyroid cancer
endometrial
Lhermitte-Duclos (brain hamartoma)
question
NF-1 increased risk of breast cancer?
answer
"moderate risk" of breast cancer
- because neurofibromas obscure real breast cancer
question
Breast cancer risk models:
- which is the best? worst?
answer
Gail model
- oldest and most validated (in African americans)
Tyrer-Cuzick
- most comprehensive
- but does not include breast density
question
is BRCA 1 or BRCA 2 more common in women? men?
answer
Women: BRCA 1 more common
Men with BRCA 2 get more cancer than with BRCA 1.
question
T/F: Breast density is an independent risk factor for breast cancer.
answer
TRUE
- denser breast, more risk
question
does exercise have any relation to breast cancer risk?
answer
Exercise decreases risk of breast cancer
- probably because of being less fat
question
What effect do the SERMs (tamoxifen and rolixifene) have on breast cancer?
answer
reduce breast cancer incidence of ER/PR positive
question
is ultrasound or stereo guided biopsy preferred?
answer
Ultrasound guided biopsy is easier
question
what size of compressed breast is needed for petite needle in stereo bx?
answer
20mm
question
size of needle for US bx
answer
14g
question
breast mass should be on the (near/far) side of the US screen? why?
answer
mass should be on the far side of the US screen
- lets you see the lenth of the needle better
question
what 4 things should line up during the biopsy?
answer
lesion, transducer, skin nick, and biopsy needle
question
what angle should the needle be when doing a biopsy?
answer
needle angle should be parallel to chest wall
- PTX as a complication is embarrassing
question
T/F: Anesthetic should be placed within the lesion.
answer
False
- should be placed up to the lesion, but not in it
question
should you biopsy the more superficial or deep part of the lesion first?
answer
biopsy the DEEP portion first
- if bleeding obscures it, you can at least get the top part
question
if you have two lesions, a big and a small one, which one should you biopsy first?
answer
the small one
- so bleeding from the big one doesn't obscure it
question
in a cystic and solid lesion, which part should you biopsy?
answer
the solid part
question
how many biopsy passes are recommended?
answer
5
question
if you put too much air inside the breast when injecting lidocaine and you can't see the mass, what is the next step?
answer
reschedule; don't try to biopsy it
question
what part of the axillary node should you biopsy?
answer
the cortex
- core biopsy is preferred over FNA
question
you suspect a hypoechoic mass is a debris filled cyst rather than a solid mass, but you aren't totally sure. what should you do first?
answer
Aspirate
question
hypoechoic mass vs cyst: you aspirate and get non-bloody fluid and lesion disappeared. what do you do next?
answer
discard the fluid; no need for cytology
- you are done
question
hypoechoic mass vs cyst: you aspirate and get bloody fluid and then lesion disappeared. next step?
answer
- send fluid to cytology
- place a clip
question
hypoechoic mass vs cyst: you aspirate and get purulent "poop like" fluid. fluid smells terrible and lesion disappeared. what do you do next?
answer
- sent it to micro lab for culture and sensitivity
question
hypoechoic mass vs cyst: you aspirate it and get fluid. the lesion does NOT disappear. what do you do next?
answer
proceed to core biopsy
question
in what situation is stereotactic biopsy used?
answer
to biopsy calcifications
- sample is xrayed after to confirm that calcs are in there
question
what type of devices are used for stereotactic biopsies?
answer
vacuum assisted
question
what should the breast compress to for stereo biopsy (compressibility of the breast)?
- why?
answer
Compressibility of the breast tissue can NOT be less than 2-3 cm (28 cm)
- you will get a "negative stroke margin"
question
___ = throw the needle to the other side of the breast into the digital receptor
answer
negative stroke margin
question
if breast compressed is too small for stereo (<20 mm), what is next step?
answer
wire localization for excisional biopsy
- or seed localization
question
clip migration after stereo is also called
answer
accordion effect
question
what are indications for a cyst aspiration? (3)
answer
- anxiety
- pain
- uncertain diagnosis
question
is size an indication for aspiration?
answer
NO
- symptoms are an indication for aspiration
question
Cysts recur about ____% of the time
answer
70%
question
how many months of mammo are required during residency training?
answer
3 months
question
recall rate should be
answer
< 10%
question
"lay reports" must be given to patients within
answer
30 days
- written results in language that is easy to understand
question
T/F: a consumer complaint mechanism is required to be established to provide patients with a process for addressing their concerns.
answer
True
question
T/F: patient can obtain ORIGINAL mammograms, not copies, when they are needed
answer
True
question
who is responsible for the Quality Control program
answer
the Interpreting physician
question
required resolution fo line pairs
answer
13 lp/mm in the anode to cathode direction
- 11 lp/mm in the left to right direction
question
what is required to pass the image quality test? (4)









")








 "very dense calcifications" in an axillary lymph node on mammo =
"very dense calcifications" in an axillary lymph node on mammo =






")





")
?")













")


?
- different distributions (3)
- what makes this suspicious?")
")
")






")


